



The midcarpal joint is the articulation between
the proximal and distal rows of carpal bones, each of which can be considered
to act as a single functional unit. The lateral part of the joint consists of
two plane surfaces which are arranged to form a slight convexity directed
distally. The larger medial part of the joint is concave distally in all
directions.
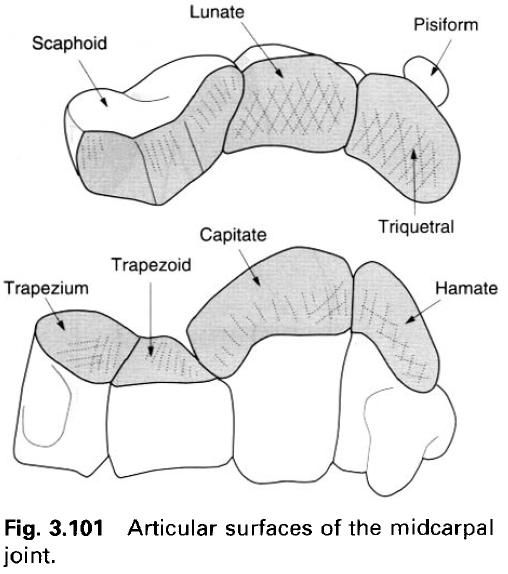
Articular surfaces
Laterally, plane joint surfaces on the
trapezium and trapezoid articulate with the slightly rounded distal surface of
the scaphoid. The head of the capitate articulates with the scaphoid and lunate
in the central part of the joint. The apex of the hamate also articulates with
the lunate, while its ulnar surface articulates with the triquetral.
Joint capsule
The midcarpal joint is surrounded by a fibrous
capsule, composed in the main of irregular bands of fibres running between the
rows of bones. Anteriorly and posteriorly these bands constitute the palmar and
dorsal intercarpal ligaments. At the sides of the midcarpal joint the capsule
is strengthened by collateral ligaments.
Intercarpal
synovial cavity
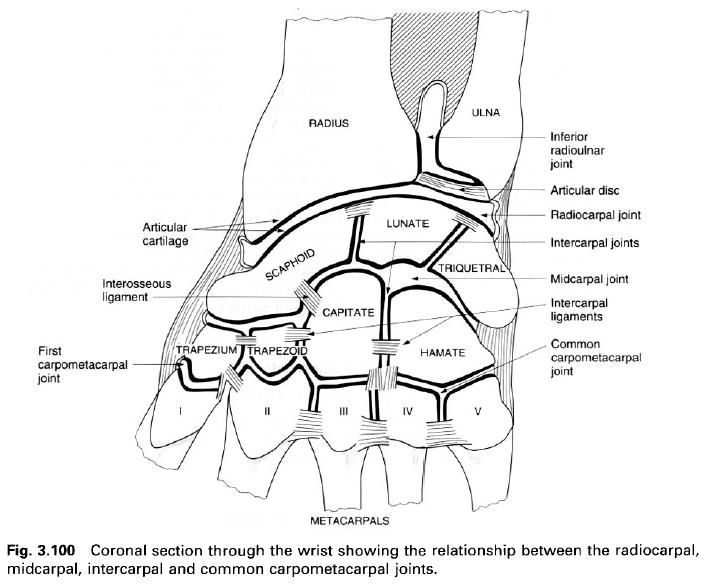
The intercarpal joint cavity is large and
complex. It extends from side-to-side between the two rows of carpal bones;
however this may be partially or completely interrupted by an interosseus
ligament between the scaphoid and capitate. Extensions of the cavity pass
proximally between the scaphoid, lunate and triquetral as far as the
interosseus ligaments between them. Rarely is there communication with the
radiocarpal joint cavity. Further extensions of the cavity pass distally
between the trapezium, trapezoid, capitate and hamate. If the interosseus
ligaments connecting these bones do not extend the full depth of the
articulation, or one is missing(usually that between trapezium and trapezoid)
then the intercarpal joint cavity communicates with the carpometacarpal joint
and is prolonged between the bases of the medial four metacarpals. The
intercarpal cavity does not, however, communicate with the first carpometacarpal
or the pisiform-triquetral joint spaces.
Synovial membrane lines the capsule and all
non-articular surfaces, attaching to the margins of all joint surfaces.
Ligaments
Palmar
intercarpal ligament

The palmar intercarpal ligament passes from the
bones of the proximal row predominantly to the head of the capitate. This
ligament is sometimes reffered to as the radiate
capitate ligament.
Dorsal
intercarpal ligament
The dorsal intercarpal ligament merely passes
from the bones of one row to those of the other.
Radial
collateral ligament
The radial collateral ligament is a strong
distinct band passing from the scaphoid to the trapezium(picture above). It is
a continuation of the radial collateral ligament of the radiocarpal joint.
Ulnar
collateral ligament
The ulnar collateral ligament connects the
triquetral and the hamate, and is a continuation of the ulnar collateral carpal
ligament of the radiocarpal joint.
Interosseus
ligament
Occasionally, a slender interosseus ligament
passes from the lateral side of the capitate to the scaphoid near its trapezoid
articular surface(picture one).
Blood
and nerve supply
The arterial supply to all the intercarpal
joints is by branches from the palmar and dorsal carpal networks.
The nerve supply to the joints is by twigs from
the anterior and posterior interosseus nerves, and the deep and dorsal branches
of the ulnar nerve; root value C7, 8.
Movements
Movements at the intercarpal joints, except the
midcarpal joint, are small, accompanying and facilitating movements at the
radiocarpal and midcarpal joints. Movements possible at the midcarpal joint are
flexion and extension, and abduction and adduction. These occur about
transverse and anteroposterior axes passing through the head of the capitate.
Flexion and extension
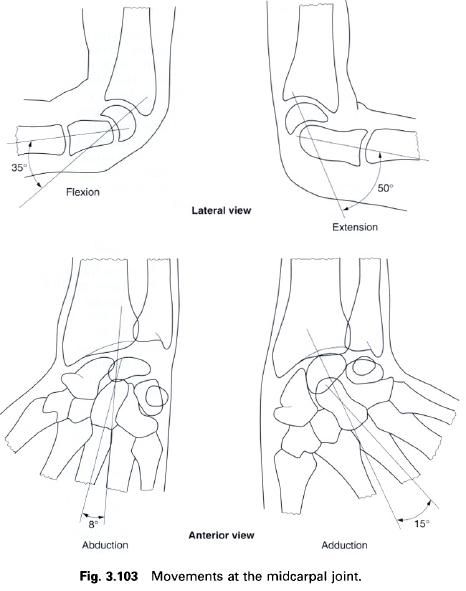
In flexion the hand moves towards the front of the forearm, while in extension it
moves towards the back of the forearm. Extension is freer than flexion, having
a range of 50°; flexion has a range of only 35°. In these movements the head of
the capitate rotates within the concavity formed by the scaphoid and lunate,
while the hamate rotates against the triquetral. Accompanying these movements
is a compensatory swing of the scaphoid on the lunate in order to receive the
head of the capitate.
Abduction and adduction
During adduction the capitate rotates so that
its distal part moves medially; the hamate approaches the lunate and separates
from the triquetral. In abduction the capitate comes close to the triquetral
separating the hamate from the lunate. Accompanying abduction and adduction is
a complex movement of torsion between the two rows of carpal bones. During
abduction the distal row of carpal bones undergoes a “rotation” in the
direction of supination and extension, while the proximal row “rotates” in the
direction of pronation and flexion. The twisting of the scaphoid delays its
impact on the radial styloid process by bringing its tubercle forwards; it also
makes the tubercle more easily palpable. In adduction a reverse twisting motion
occurs so that the proximal row “rotates”
in the direction of supination and extension, while the dorsal row moves
in the direction and flexion. It must be emphasized that these movements are of
extremely small magnitude. It is debatable whether they contribute much to the
normal functioning of the wrist.
The range of abduction and adduction are 8° and
15° respectively. The principal limit to abduction is a closing of the lateral
part of the joint space between the scaphoid and the trapezium.
Accessory
movements
Anteroposterior gliding movements of any two
adjacent carpal bones can be produced if one is stabilized while the other is
moved. This can be achieved by gripping each bone between the thumb and index
finger.
Anteroposterior movement at the midcarpal joint
can be elicited using a similar technique to that described for the radiocarpal
joint. A firm circular grip is applied around each carpal row. While the
proximal row is stabilized, the distal row can be moved anteroposteriorly.
Applying the same grip, a longitudinally applied force separates the two joint
surfaces.











0 коментара:
Постави коментар